|
November 2, 2016
By Andy Slavitt, CMS Acting Administrator (@aslavitt) and Patrick Conway, MD, MSc, CMS Acting Principal Deputy Administrator and Chief Medical Officer
A
Healthier Medicare: Focusing on Primary Care, Mental Health, and Diabetes
Prevention
We’ve discussed a number of times how our country’s health
care system historically invested far more in treating sickness than
maintaining health. This imbalance contributes to more spending on
institutions, hospitals, and nursing homes, rather than keeping people
healthy at home and in their communities.
By better valuing primary care, care coordination and
prevention, we help people access the services they need to stay well. In
addition to keeping people healthy, health care costs are often lower when
people have a primary care provider and team of doctors and clinicians
overseeing and coordinating their care. And efforts to reduce documentation
burden in care management and coordination, tied in with our strategy of physician and clinician engagement,
helps keep the focus on patient care that pays for what works and better
supports and engages the medical community.
That’s why Medicare and Medicaid, with invaluable support from
the CMS Innovation Center, have implemented policies to sharpen their focuses
on individuals and their care. Continuing that work, today, Medicare is finalizing
policies that improve how it pays for primary care, care coordination, and
mental health care, and expanding an exciting CMS Innovation Center payment
and service delivery model that aims to prevent diabetes.
Preventing Diabetes & Protecting the Medicare Trust Fund
About 26 percent of people 65 years or
older, more than 11 million people, have diabetes. They face higher risks of
debilitating complications like heart disease, kidney failure, limb
amputations, and blindness. And the treatment of people with diabetes is
expensive. It costs Medicare more to support care for those with diabetes
than those without diabetes. In total, we estimate that Medicare will spend
$42 billion more in the single year of 2016 on fee-for-service, non-dual
eligible, over age 65 beneficiaries with diabetes than it would spend if
those beneficiaries did not have diabetes -- $20 billion more for Part A, $17
billion more for Part B, and $5 billion more for Part D.
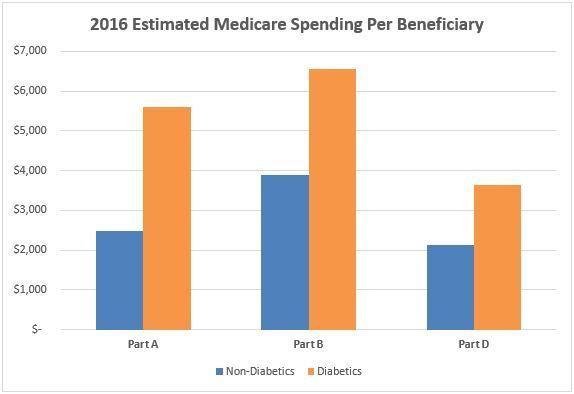
On a per-beneficiary basis, this disparity is just as clear.
In 2016 alone, Medicare will spend an estimated $1,500 more on Part D
prescription drugs, $3,100 more for hospital and facility services, and
$2,700 more in physician and other clinical services for those with diabetes
than those without diabetes. That’s approximately $7,300 or 86 percent more per
beneficiary, per year for someone with diabetes. This increased spending
reflects only Medicare’s share of costs; diabetic beneficiaries likely
experience higher out-of-pocket spending as well. Taking care of people with
diabetes is important, which is why Medicare provides quality services and
support to those with diabetes.
 |
|
But
what if we could slow – or even reduce – the number of people developing
diabetes in the first place? What if by focusing on primary care and
prevention, we could help people live healthier lives while reducing the
costs to the health system and beneficiaries.
The
Diabetes Prevention Program model test set out to test this idea.
Participants at high risk for developing diabetes were provided strategies to
increase their physical activity, control their weight, and decrease their
risk of type 2 diabetes. This model led to approximately 5 percent reduction
in weight and saved Medicare an estimated $2,650 for each person enrolled in
the Diabetes Prevention Program model test over a 15-month period, more than
enough to cover the cost of the program.
The
Medicare Diabetes Prevention Program (MDPP) expanded model, set to begin in
2018, hopes to make these services available to all eligible Medicare
beneficiaries, improving their health and that of the Medicare program both
now and in the future. We know that fewer people with diabetes saves patients
and Medicare money because they use fewer expensive prescription drugs and
have fewer hospital visits. And most importantly, by preventing diabetes,
patients and families across the country can avoid suffering from a
debilitating disease. That’s why we are expanding the model to make MDPP
services available to all eligible Medicare beneficiaries.
The
Medicare Diabetes Prevention Program expanded model is the latest successful
effort at the Innovation Center to inform the evolution of the Medicare
program over time. Other Innovation Center models have tested new ways for
doctors and hospitals to work together to support and coordinate care for
their patients and better patient safety. Models are eligible for expansion
under Section 1115A(c) of the Social Security Act if they meet the following
criteria: First, the Secretary of the Department of Health and Human Services
determines that such expansion is expected to improve quality of patient care
without increasing spending or reduce spending without reducing quality of
patient care. Second, the independent CMS Chief Actuary must certify that the
expanded model would reduce or not result in any increase in net program
spending. Third, the HHS Secretary determines that such expansion will not
deny or limit the coverage or provision of benefits Medicare beneficiaries
receive. The Medicare Diabetes Prevention Program expanded model meets these
criteria.
Refocusing
Medicare on Primary Care and Behavioral Health
Also,
today, Medicare announced an important set of changes that would improve how
Medicare pays for primary care, care coordination, and mental health care.
These changes will result in an estimated $140 million in additional funding
in 2017 to physicians and practitioners providing these services. Over time,
if the clinicians qualified to provide these services were to fully provide
these services to all eligible beneficiaries, the increase could be as much
as $4 billion or more in additional support for care coordination and
patient-centered care.
Clinicians will
additionally be able to bill and be paid more appropriately when they spend
more time with their patients,
serving their patients’ needs outside of the office visit, and
better coordinating care. These changes are designed to improve
health outcomes. With today’s final primary care payment policies, Medicare
continues to move toward a health care system that encourages teams of
clinicians to work together and collaborate in order to provide
more personalized care for their patients.
Geriatricians,
internists, and family physicians provide core services for the Medicare
program, including the kinds of care management and patient-centered care
that are described by these new codes. Over time, we estimate that the
payment increases attributable to these new codes could be as much as 30 and
37 percent respectively to these specialties.
We
are also finalizing new coding and payment for care using the Psychiatric
Collaborative Care Model that supports mental and behavioral health through a
team-based, coordinated approach involving a psychiatric consultant, a
behavioral health care manager, and the primary care clinician and which
extends beyond the scope of an office visit. This care model has been shown to
improve behavioral health outcomes for patients and save money. Payment
for care using this model will help address one of the health system’s major
challenges -- access for behavioral and mental health care. For anyone
who has struggled to gain access to behavioral health care for themselves or
a loved one, the importance of these services cannot be overestimated.
Strengthening
Primary Care beyond Medicare
As
more people age into the Medicare program, we know that access to primary
care is an essential tool for their health and wellbeing. We know that
effective primary care, care coordination and planning, mental health care,
substance use disorder treatment, and care for patients with cognitive and
functional impairments can improve outcomes and result in smarter spending.
Today’s changes are part of CMS’s broader goal to improve how we pay for
care, including through our recently announced Quality Payment Program for Medicare physicians.
We
expect to see the impact of these policies far beyond Medicare beneficiaries
and hope that they will help strengthen the fabric of primary care throughout
the country.
For
more information, please visit: https://www.cms.gov/Newsroom/MediaReleaseDatabase/Press-releases/2016-Press-releases-items/2016-11-02.html and https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-11-02.html.
###
Get CMS news at cms.gov/newsroom, sign up for CMS news via email and follow CMS on
Twitter @CMSgovPress
|

At Medicare is Simple, we look to educate and enable you to choose among Medicare plans to help find the policy that may best fit your needs. Get free quotes using our advanced quoting technology. HealthCare Reform is also a hot topic of interest to people of all ages, and we look to keep you updated on the issues relevant to learning more. Medicare Is Simple 800-442-4915
Friday, November 4, 2016
A Healthier Medicare: Focusing on Primary Care, Mental Health, and Diabetes Prevention
Subscribe to:
Post Comments (Atom)
No comments:
Post a Comment